
Hospital Birth Guide
Illustrations from The Educated Birth.
Let’s talk about birth plans! What is a birth plan, and how can we possibly plan for birth? First, I like to call it birth preferences or a birth guide. Ultimately, our goal is to become as educated and informed as possible prior to the start of your birthing time, so that you have fewer decisions to make and can focus on the work your body needs to do to birth your baby. Birth is wildly unpredictable, and we can only do so much to influence it, so look at this as sort of a flow chart; if this happens, I would like this type of thing. Throughout this guide, we’ll explore your preferences for labor, birth, and postpartum. Once we have explored all of these essential questions, we will create a 1-2 page document that we use as a communication tool with your care team during your birthing time, which is the main purpose of a “birth plan,” birth preferences, birth guide, or whatever language prefer. you
Let’s start by talking about what you can expect when you’re planning to give birth at a hospital. Some of these things may vary and depend on your individual history and risk profile. In my experience as a doula, hospitals in the Bay Area are pretty good at staying up to date and providing evidence-based, patient-centered care. One reason is that most hospitals follow a set of guidelines from the California Maternity Quality Care Collaborative (CMQCC).
“California Maternal Quality Care Collaborative (CMQCC) is a multi-stakeholder organization committed to ending preventable morbidity, mortality and racial disparities in California maternity care. CMQCC uses research, quality improvement toolkits, statewide outreach collaboratives and its innovative Maternal Data Center to improve health outcomes for mothers, birthing persons and infants. CMQCC was founded in 2006 at Stanford School of Medicine together with the State of California in response to rising maternal mortality and morbidity rates. Since CMQCC’s inception, California has seen maternal mortality decline by 65 percent between 2006 to 2016, while the national maternal mortality rate continued to rise.”
CMQCC provides several toolkits and algorithms to hospitals to increase rates of vaginal birth, decrease rates of primary cesareans, address hemorrhage, and manage infections and sepsis safely.
CMQCC sets a standard that hospitals should follow a shared decision-making model, where patients and their providers weigh risks and benefits collaboratively, without coercion. Other ways that hospitals can support good outcomes for families are by promoting freedom of movement in labor, eating and drinking as the patient desires, providing or supporting the use of alternative measures of pain management (showers, tubs, peanut balls, nitrous oxide, TENS units, and more), addressing fetal, providing intermittent auscultation as the standard of care for low-risk birthing people, and much more! You can learn more about CMQCC at cmqcc.org.
While shared decision making is emphasized, it is important to note that sometimes providers are beholden to hospital policy, which is often dictated by a fear of litigation. In some circumstances, you may be provided a recommendation that is not evidence-based or doesn’t take into account your personal clinical picture. At any time, you have the right to informed consent and informed declination. Hospital policy is not the law, and you cannot be punished for choosing something against medical recommendation or advice. Birth Monopoly is a great site to visit to learn about your rights in childbirth.
Let’s move on to discussing birth choices now.
I have a template linked here for creating your birth preferences. This goal of this guide is to help me understand your preferences, as one of your support people. Not everything that we discuss is necessary to put on your birth preferences, as the primary purpose of that document is as communication tool with staff. For example, we may have plans to use aromatherapy in labor, but the staff isn’t going to be participating or helping with that, so there isn’t a reason to write it. We don’t want to bog down your plan with unnecessary details so that the important details are remembered. You can access the template now, or you can wait until after you have finished reading the materials to create your birth guide.
To use this template, click the link. It will take you to a Google Doc. Select file > Make a copy. It will take you to your google document in a new tab.
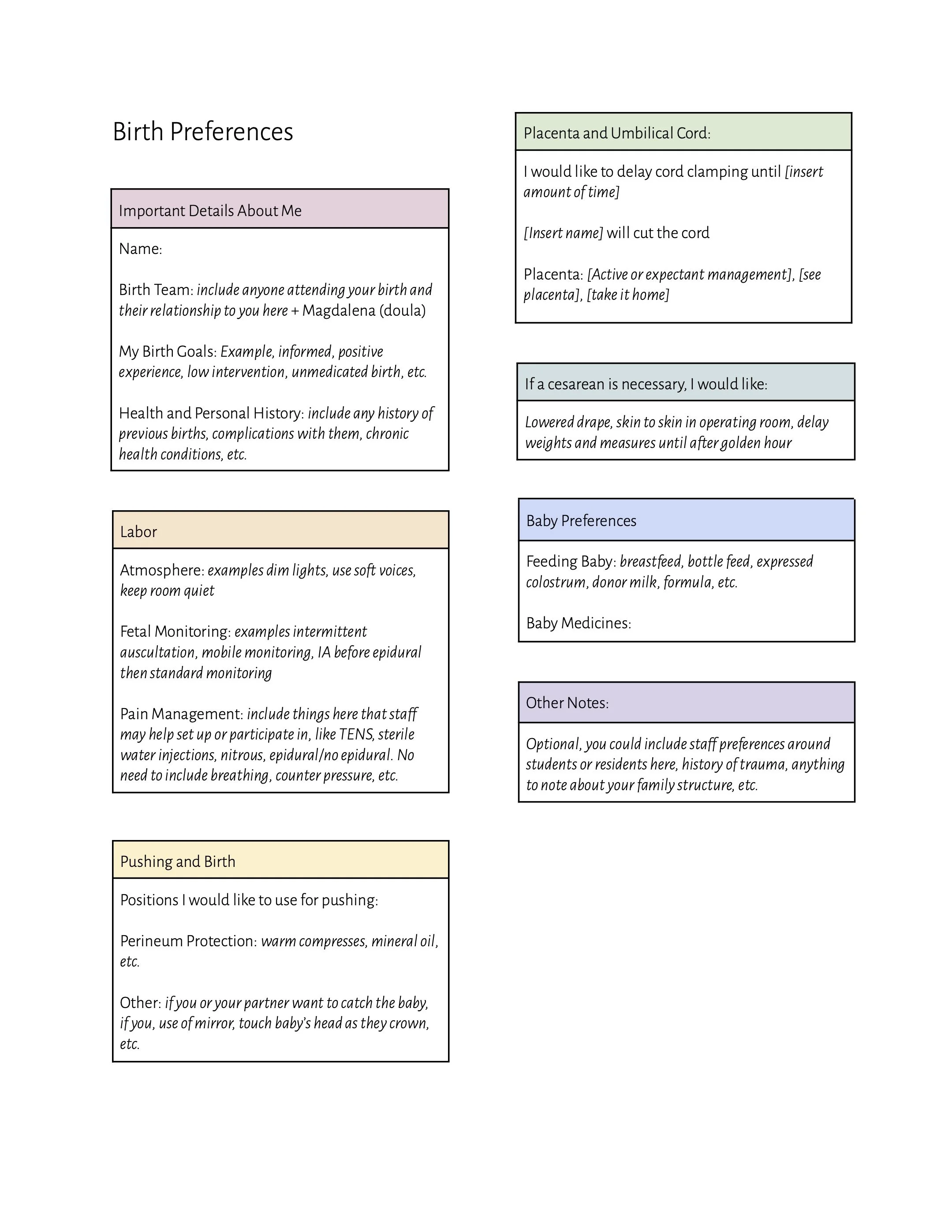
Birth Preferences Example
I have a template linked here for creating your birth preferences. This goal of this guide is to help me understand your preferences, as one of your support people. Not everything that we discuss is necessary to put on your birth preferences, as the primary purpose of that document is as communication tool with staff. For example, we may have plans to use aromatherapy in labor, but the staff isn’t going to be participating or helping with that, so there isn’t a reason to write it. We don’t want to bog down your plan with unnecessary details so that the important details are remembered. You can access the template now, or you can wait until after you have finished reading the materials to create your birth guide.
To use this template, click the link. It will take you to a Google Doc. Select file > Make a copy. It will take you to your google document in a new tab.
Staff Preferences
How do you feel about students or residents being involved in your care? Please note if you would decline the presence of any of the following:
Resident doctors are graduates of medical school who are in training under the supervision of board-certified doctors (attending physicians) or certified nurse midwives and often co-manage your care with their supervisor. They may perform cervical exams, make recommendations, or be the primary person involved in delivery.
Student midwives may also be a part of your care team. Student midwives are registered nurses in the final stages of their clinical training to become Certified Nurse Midwives and may play a similar role to residents, often co-managing your care, performing exams, and catching your baby.
Medical students and nursing students are often observers during birth, and do not perform procedures.
Are you comfortable with male providers and staff being present during your labor and birth? If there are some scenarios where it would feel comfortable, but some not, list them.
Fetal Monitoring
Labor is a stressful event for both you and baby, but you are both built to do this! Babies have reserves to handle the stress of labor, to a certain extent. The only tool we have to know how the baby is doing is through monitoring their heartbeat. We have a few ways to do this. Read the Evidence on: Fetal Monitoring.
Intermittent auscultation with a handheld Doppler is the most evidence-based option for those with low-risk pregnancies. When you request intermittent monitoring, hospitals typically require 20 minutes of continuous monitoring (called a strip, or non-stress test). From there, they can look at a picture of how baby is doing, and if baby is well, perform intermittent monitoring for the rest of the labor. During early labor, they typically listen to baby hourly. As you progress to active labor they listen every 30 minutes, and more frequently as you get close to pushing your baby out. Examples of situations that would risk you out of intermittent monitoring include gestational hypertension, twins or multiple pregnancies, cholestasis, Pitocin augmentation, and epidural use.
Continuous monitoring is when your baby’s heartbeat and your contractions are constantly monitored throughout your labor. Typically this is done with a cardiotocography (CTG) machine, which involves two monitors being placed on your abdomen, one higher for detecting your contractions, and one lower for your baby’s heart beat. These monitors are connected to the CTG with wires, so mobility is limited. Some hospitals have telemetry units, where the wires are connected to a small CTG that can be carried around. The other continuous monitoring option is Bluetooth monitoring, which involves a sticker with electrodes being stuck to your abdomen, and you are wire free. This option offers more mobility when continuous monitoring is required.
Non-routine: In some circumstances, baby’s heartbeat may not be able to be consistently and accurately traced from the outside of your body. In higher risk situations where continuous monitoring is indicated, you may be recommended to have an internal monitor placed, called a fetal scalp electrode (FSE). This is a small wire that is placed just under the skin of your baby’s scalp and provides a highly accurate tracing. Your water must be broken for an FSE to be placed.
Pain Management
Pain management is a big part of birth preparation and your birth preferences. Whether or not you choose to birth unmedicated (without an epidural), creating a toolkit of pain management techniques is important. Using other techniques to manage pain and delaying epidural usage (even if you plan to get one) is an evidence-based strategy for decreasing rates of intervention. It is also possible that you receive an ineffective epidural, in which case it will also be crucial to have other options.
Many people have strong feelings about their plan to use or not use an epidural for pain management. I encourage you to explore your own feelings about epidurals by choosing a number on this scale:
0: You would refuse pain medication in every circumstance, even in emergent scenarios (impossible extreme).
1: You have a very strong desire for an unmedicated birth, you will be disappointed by your birth experience if you end up needing an epidural and would likely only accept it in extreme circumstances.
3: Your preference is for an unmedicated birth, and you would like to utilize all other strategies before considering an epidural, but would accept one in certain circumstances, like a prolonged labor or induction.
5: Unattached to either receiving or not receiving an epidural. You might like to see what your body can do on its own, and explore the sensations of birth, but if you’re not coping well, you would ask for an epidural and feel happy with that choice.
7: You plan to get an epidural after utilizing other pain management strategies first. If your birth went too quickly for an epidural, you wouldn’t be disappointed or upset that you couldn’t receive one.
9: You have a strong preference to use an epidural. You might use other coping techniques at home before active labor. As soon as active labor begins, or as soon as you arrive at the hospital, you would like to receive one. You would be upset if you did not get an epidural.
10: You desire to feel no pain in childbirth (impossible extreme).
Listen to the Evidence Based Birth® Podcast episode on Epidurals for Pain Management.
What are your thoughts and feelings about epidurals in labor? What questions do you have? Please write down your answer below so we can discuss it!
Evidence Based Birth® has a pain management series on YouTube that access here. All of the options listed here can be found on this playlist. Please write down any questions or thoughts you have about any of these.
Acupuncture or Acupressure
Quiet Room
Soft Voices
Dim Lighting
Conscious or Guided Breathing
Hypnosis or Meditation
Massage, Counter Pressure, and Hip Squeezes
Music
Frequent Movement
Sterile Water Injections
TENS Unit
Shower or Tub
Words of Affirmation
Injectable opioids
Nitrous oxide
Cervical Exams
Dilation is usually thought of as the key measure of progress in labor, but it really doesn’t tell us much at all. I have had clients walking around at 4cm for weeks, and I have had people who were 2cm and gave birth an hour later. The cervix shows us a single snapshot in time, and does not tell us when baby arrives. They are also uncomfortable for many people, and with each check after your water has broken you risk of infection increases. These are the main reasons we try to minimize cervical exams. Hospital policy dictates that providers typically recommend performing an exam on admission, every 4 hours while in active labor, and before beginning pushing. It is within your right to decline any of these checks. If you have questions about cervical exams, please note here.
Vital Measurements
A set of vitals is taken at your consent when you arrive at the hospital, and every 4 hours while you are in active labor. This includes your pulse rate, oxygen saturation, blood pressure, and temperature. Once your waters have broken, they may check your temperature every 1-2 hours to ensure you do not have a fever, signifying infection. Vital sign checks are a non-invasive way to ensure you are stable, which also tells us more about your baby’s condition. Your nurse will ask for consent before doing these checks and will make an effort not to perform them during a contraction.
Saline Locks and IV Medications
A saline lock is an IV port that is placed and capped, so that IV access is available, but you are not connected to anything. A saline lock may be used for IV hydration during labor, antibiotics for Group B Strep or chorioamnionitis (infection in the uterus), Pitocin augmentation or induction of labor, and administration of antihemorrhagic drugs after you give birth. Some people with low-risk profiles who are also planning to decline routine 3rd stage Pitocin may consider declining a saline lock. If you’d like to discuss risks and benefits of this routine intervention, please note here.
Non-Routine Interventions in Labor
Artificial Rupture of Membranes (AROM) is when a provider uses a hook shaped tool, comparable to a crochet hook, to break your bag of waters during a cervical exam. In the vast majority of births, this is not necessary, but it can be a useful tool. If labor has slowed or stalled, AROM is a non-pharmacologic (drug free) way to augment, or speed up labor. Risks of AROM are increased risk of infection and cord prolapse, which is when the cord slips in front of the baby’s head, and the baby’s head applies pressure to the cord, kinking it like a hose. This is an obstetric emergency that requires immediate cesarean. We can mitigate these risks by not breaking water early in labor, and ensuring that baby is engaged in the pelvis and the head is well-applied, so the cord cannot slip through.
Intrauterine pressure catheters (IUPC) are most often used during Pitocin augmentation or induction. An IUPC is a thin tube that is placed by a provider through the vagina, cervix, and into the uterus next to your baby. External contraction monitors do not tell us the strength of contractions, only if they are happening. An IUPC tells us how much pressure your uterus is generating during contractions, which can help your team more carefully dose your Pitocin to ensure contractions are effective, while also not making them too strong. An IUPC comes with a higher risk of infection.
An amnioinfusion is when sterile saline is put into the uterus via an IUPC. This may be recommended if your baby is having a specific kind of deceleration (heart rate drop) that tells us there is umbilical cord compression (the hose is being kinked), which affects your baby’s ability to stay well oxygenated. An amnioinfusion helps this issue by creating more buoyancy around the cord with fluid, so there is less compression.
Pushing and Birth
Pushing your baby out can look many different ways. If you are unmedicated, you will likely feel an undeniable urge to bear down and require little guidance to get your baby birthed. If you have an epidural, it may lengthen the pushing stage significantly and require a more coordinated effort to push your baby out. When it is your first time giving birth, it is typical for it to take 1-3 hours from the time you begin pushing until baby is born.
You have many options for how you’d like to push and deliver your baby. Utilizing different positions is an evidence-based strategy for decreasing pushing time. Gravity is also a useful tool for bringing baby down.
Warm compresses are a great way to reduce your risk of tearing. A warm washcloth on your perineum increases blood flow to the area and encourages your tissues to stretch and accommodate baby. You can also request a mirror to see baby as they are being born, or touch baby’s head as they crown. I find that it is very motivating to do either or both of these during pushing!
You, your partner, or another important person may assist with delivering the baby. I find that most providers are very open to this. The provider typically ensures the head and shoulders, and coaches your partner to grab baby under the arms and bring baby up to your chest. If this is something you’d like to do, please note here!
Non-Routine Interventions during Pushing and Delivery
A vacuum is a suction device placed on baby’s scalp. It is then pulled on by a provider to expedite delivery. It is used in cases of exhaustion or fetal distress. It can only be used if baby’s head is low enough to be visualized. It comes with an increased risk of tearing for the parent and a risk of a scalp hematoma for the baby.
Epidurals do increase rates of vacuum and forceps delivery. Forceps are not used in hospitals in this area.
An episiotomy is an incision in the perineum. They are not used routinely because the risk of severe tearing is higher with an episiotomy, and they typically are more difficult to heal than a natural tear. In this area of the country, episiotomies are only used in emergent situations like fetal distress, where delivery must be expedited, and shoulder dystocia, an obstetric emergency where the shoulder is stuck behind the pubic bone after the head has delivered.
The Golden Hour and Third Stage of Labor
After baby is born, they are placed on your belly or chest. Most babies get a good rub with a warm blanket to stimulate them to cry, but the vernix is left on baby. The golden hour is the first hour of baby’s life after they are born. Hospitals support immediate skin-t0-skin, which is proven to regulate baby’s body temperature, blood sugar, and is bonding time for you and your baby! Nursing is initiated during this first hour when baby is alert and ready to feed. Your care team will perform baby’s vital checks while baby is skin to skin with you.
During this time, you also have to deliver your placenta. Typical hospital management of the third stage (the time between your baby’s birth and the birth of the placenta) involves active management, which is Pitocin and cord traction. Please read Evidence on: Pitocin and decide if an active management or expectant management is your preference. These terms are defined in the handout. Circle here if you’d like expectant management or active management.
Many hospitals provide delayed cord clamping, though their definition of this may range from 30 seconds to 30 minutes or longer. Baby receives the most benefit in the first 2 minutes, but many families choose to wait for the cord to stop pulsing, or turn flat and white, to ensure baby has received as much of their blood as possible. Some parents may choose to leave the cord and baby attached until after the placenta is born and clamp and cut later. There is no medical need to rush clamping and cutting the cord. Please write your preferences for clamping the cord, and who will cut the cord below.
What are your thoughts about your placenta? Is there anything you’d like to do to appreciate it? See it? Touch it? Take it home? There is a handout in your binder all about the placenta and different options of what you can do with it. Please write any plans or questions about your placenta below.
Cesarean Birth Preferences
A family-centered cesarean is an approach to cesarean birth that promotes birth being a sacred, important moment for a family, even if it’s happening in a bright operating room. You may also hear them called gentle cesareans. What matters most, no matter how you birth, is that you are the one who is empowered to make the choices that are safest for you and your baby. I have listed out some options of things people commonly ask for during their cesarean births, either planned or unplanned.
In the illustration above, the drape is lowered as baby is born, so that the birthing person can see their baby.
Options you have in a non-emergent cesarean:
Support person in the operating room
No arm restraints
Procedure explained as it is happening
Birth-focused conversation from staff in the operating room
Staff members introduce themselves before beginning the procedure
Music of choice
Gentle cesarean: baby born slowly through incision to mimic the vaginal “squeeze” and provide a slower entry to the outside world
Delayed cord clamping
The cord to be left long so you or your partner can trim it
Lowered drape as baby is born (you do not see the surgery or incision site)
Clear drape
Skin-to-skin in the OR
No weights, measurements, or medicines until after the golden hour
Vaginal seeding
Help with initiating nursing in the operating room if baby begins cueing to feed
Feeding Your Baby
Human milk is the most optimal nutrition for your baby. Health benefits, compared to formula, include lower risks of SIDS, allergies, and obesity and diabetes later in life. Nursing may not be an option for every family, but I encourage you to explore the option of donor milk if you cannot produce milk. Hospitals have donor breastmilk for anyone who needs it.
I may have clients who have an oversupply and will happily connect you if you would like donor milk. There are often people in the community willing to donate milk if you ask!
If you are planning to nurse, I highly recommend expressing colostrum before labor to develop this skill and to have a bit of extra milk just in case baby has blood sugar issues. Most hospitals have a freezer for this purpose and will keep your colostrum there while you are in labor. If you have questions about expressing colostrum, please let me know.
Please write below your plans for feeding baby and any feelings, questions, or concerns you have about feeding your baby.
Baby Medications and Procedures
There are 3 medications recommended for all newborns in the first two hours of life: Vitamin K injection, erythromycin eye ointment, and Hepatitis B vaccine.
Read Evidence on: Vitamin K for Newborns and Evidence on: Eye Ointment. Vitamin K is a clotting factor that babies are unable to produce on their own, so an injection is recommended to prevent life-threatening bleeding. The eye ointment is primarily to prevent infections from gonorrhea or chlamydia that may cause permanent blindness.
Other procedures and tests that take place before discharge include a metabolic blood screen, bilirubin testing, a hearing test, a pulse oximeter test for congenital heart defects, and circumcision if you choose. Read Evidence on: Circumcisionif you are considering circumcision for your child.
Which baby medications do you plan to accept or decline? Do you have any questions about newborn procedures and tests?
Induction or Augmentation Birth Preferences
Please read the handout on the Evidence on: Inducing for Due Dates.
If you and your baby are healthy and the pregnancy is proceeding as expected, when would you prefer induction if you haven’t gone into labor on your own?
Options:
Electively between 39–40 weeks*
Electively between 40 weeks and 40 weeks + 6 days*
At 41 weeks exactly
Between 41 weeks and 1 day to 41 weeks and 4 days
As long as possible (41w5d–42w)
*Elective induction availability is often determined by the beds and/or staff a hospital may have. Individuals who request an elective induction may be put on a waiting list.
Please read Evidence on PROM (Pre-labor Rupture of Membranes) so that you are aware of the risks and benefits of waiting versus inducing labor if your water breaks without contractions beginning.
Read or listen to the Evidence on Membrane Sweeping by using this QR code.
Options you may consider for membrane sweeping:
I would like to receive membrane sweeps between 39-40 weeks
I would like to receive membrane sweeps between 40-41 weeks
I would like to receive membrane sweeps only after 41 weeks to avoid a medical induction
Or
I am not interested in membrane sweeping
We will discuss different induction methods together in-person and I will provide the evidence on different forms of cervical ripening: misoprostol, dinoprostone, or mechanical balloons. We will discuss methods that may be used for induction or augmentation: artificial rupture of membranes, and Pitocin (low-dose versus high-dose protocols).